Adenoviruses have been used in gene therapy and have also been researched for use in vaccines for decades. An adenovirus-based vaccine was authorized for emergency use to fight COVID-19 in the U.S., along with the two mRNA vaccines. We can build protection against the virus in our communities if enough people are vaccinated. Learn more about how the adenovirus-based vaccine works and find answers to many common questions below.
What is COVID-19?
COVID-19 is an infectious disease caused by a strain of coronavirus discovered in 2019, called SARS CoV-2. The disease is typically spread through respiratory droplets in the air from an infected person. SARS CoV-2 causes a range from no symptoms (asymptomatic) to severe symptoms, including fever, cough, fatigue, and breathing difficulty. Coronaviruses are a family of viruses that cause a number of different diseases, including COVID-19. The COVID-19 outbreak is defined as a pandemic, because it has spread across multiple countries and has affected a large number of people.
What are adenoviruses?
Adenoviruses are a group of viruses that cause common illnesses and symptoms, like fevers and coughs. The Johnson & Johnson (J & J) vaccine for COVID-19 is made using a specific type of adenovirus called adenovirus type 26 (Ad26). Scientists have learned how to disable genes that can cause illness while keeping the ability to get into cells to treat or prevent disease. This means that the engineered “virus” used in the vaccine cannot replicate, or make copies, in the human body to cause illness.
.aspx?width=350&height=350) How does an adenovirus-based vaccine work against COVID-19?
How does an adenovirus-based vaccine work against COVID-19?
An adenovirus can be used as a vector, or carrier, to deliver a gene to cells with instructions to make a protein that are required for the body to function properly. Think of the adenovirus vector as an envelope with a message inside. In the case of a vaccine to fight COVID-19, the message being delivered is a gene that will instruct cells to temporarily make just enough of the SARS CoV-2 spike protein to activate the immune system. The cells are not given enough instructions to build the full virus so the vaccine cannot cause COVID-19. This spike protein is an antigen that is recognized by the immune system as a foreign invader. These antigens trigger the immune system to produce specific protective antibodies that neutralize the virus— in this case, the antibodies needed to fight COVID-19.
If a person is exposed to SARS-CoV-2 after receiving the vaccine, the immune system will detect the familiar antigens and produce antibodies to attack them. A vaccinated person’s immune system can better defend against the infection altogether or greatly reduce the severity of the infection.
How many doses are required?
The adenovirus-based vaccine for COVID-19 was authorized to be given in a single dose. There is another clinical trial under way to test the effects of two doses, but the results of the trial are not expected until May.
What are clinical trials?
Clinical trials are a required step in the research process that studies the way an intervention interacts with the body. Clinical trials typically take many years and are divided into different phases that answer specific questions about the treatment, primarily whether it is safe and effective. However, the FDA has created expedited pathways and programs to accelerate the process while still maintaining high standards. This is typically done for drugs and therapies for serious diseases with no other treatment options, or for public health emergencies— fitting for interventions that fight COVID-19.
Who is eligible to receive the vaccine?
 Everyone 16 years and older is now eligible for COVID-19 vaccines. Visit the CDC’s Covid-19 Vaccine Rollout Recommendations to learn more and to select your state to see the state’s plan.
Everyone 16 years and older is now eligible for COVID-19 vaccines. Visit the CDC’s Covid-19 Vaccine Rollout Recommendations to learn more and to select your state to see the state’s plan.
Do I still need to get vaccinated if I already had COVID-19?
Yes. The CDC recommends getting vaccinated even if you have already had COVID-19, because you can get infected more than once. You may have short-term antibodies for protection after recovering from COVID-19, but we don’t know how long this protection lasts. Also, there were no concerns reported from the clinical trials if a participant had COVID-19 and was also vaccinated.
Are there certain people who should not receive the vaccine?
Very few, but individuals with known history of a severe allergic reaction (e.g., anaphylaxis) to any component of the COVID-19 vaccine should not receive the vaccine. Speak with your doctor to make the decision if:
- You are immunocompromised, meaning you have a known impaired immune system
- You have a bleeding disorder or are on a blood thinner
- You are pregnant or breastfeeding
- You have a history of severe allergic reaction such as anaphylaxis to any vaccine or injectable therapy
- You are currently a participant in a gene therapy clinical trial or plan to in the future
This vaccine is currently not being given to children under the age of 18. But it is being studied in pediatric clinical trials to understand whether it will be safe and effective for younger ages.
If I have a rare disease, will the adenovirus-based vaccine affect my eligibility to receive gene therapy in the future?
Speak with a provider to carefully consider if an adenovirus-based vaccine is right for you. Gene therapy treatments often use a viral vector to deliver a working gene. However, there is concern that being exposed to a specific virus could build natural immunity and therefore would make treatment using a viral vector ineffective.
If I am currently a participant in a gene therapy clinical trial, can I get the vaccine?
Check with your provider of the gene therapy trial before receiving the vaccine.
How effective is the adenovirus-based vaccine?
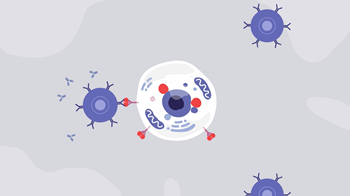
The adenoviral vector enters the cell to trigger an immune response to build antibodies.
The J & J clinical trials for the adenovirus-based vaccine had positive results. The clinical trials data are from 43,783 participants in the U.S., South Africa, certain countries in South America, and Mexico who did not have evidence of SARS-CoV-2 infection prior to receiving the vaccine. Of the 21,895 participants that received the vaccine, it was found to be 66 percent effective at preventing moderate to severe COVID-19 from occurring at least 28 days after vaccination. Even better, the vaccine was able to reduce the risk of adults getting severe or critical disease by 85 percent and offered complete protection against COVID-related hospitalizations and deaths. At this time, data is not available to determine how long the vaccine will provide protection. However, having protection for any length of time from the vaccine could be beneficial over no protection. Getting vaccinated may also protect people around you, particularly people at increased risk for severe illness from COVID-19.
Are there any side effects of this vaccine?
Like any medical intervention, vaccines can cause side effects, which are potential effects known from studies to be caused by a certain vaccine. Side effects are a type of adverse event. An adverse event is any health problem ranging from minor to serious, that happens after vaccination, whether it is caused by the vaccine or not. During testing of the adenovirus-based vaccine in clinical trials the participants that received the vaccine were followed for about eight weeks after vaccination. The most reported side effects were pain at the injection site, headache, fatigue, muscle aches, and nausea. Most of these side effects were mild to moderate in severity and lasted 1-2 days. This often means that your immune system is doing its job. Call your doctor if you have any symptoms that concern you after you are vaccinated.
Since authorizing the use of the J&J vaccine, the FDA and CDC recommended a 10-day pause in providing this vaccine to allow time to investigate an adverse event of thrombosis with thrombocytopenia syndrome (TTS) that occurred after vaccination in a total of 15 cases out of over 7 million doses given. The FDA has now determined from the available data that the vaccine’s known and potential benefits of the J&J vaccine in preventing COVID-19 outweigh its known and potential risks in individuals 18 years of age and older. At this time, the available data suggest that the chance of TTS occurring is very low.
Will the vaccine stop me from spreading the virus to others?
At this time, there is no evidence of whether the vaccine prevents transmission of SARS-CoV-2 from person to person. Clinical trial data show that these adenovirus-based vaccines do a very good job at preventing symptomatic COVID-19. But data is still being collected to understand how well the vaccine prevents asymptomatic infection (infection without symptoms). Research is ongoing to determine whether a vaccinated person might still be able to transmit COVID-19 to someone else who is not vaccinated. This is why it is important for a large proportion of the population to be vaccinated.
Will the vaccine change my DNA?
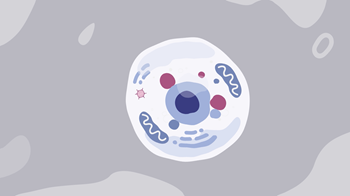
The adenoviral vector in the cell does not travel to the cell’s nucleus.
No, the adenovirus-based vector used for the vaccine is non-integrating. That means the DNA (or gene) they carry won’t insert itself into the cell’s genome. So, if the viral vector is taken up by a cell that divides, the gene won’t be copied with each cell division and will be lost over time. The adenoviral vector carrying the gene is only in the body long enough to its job of building antibodies, will eventually be cleared out, and won’t change a person’s DNA.
How does a vaccine help build herd immunity?
 Vaccinations and herd immunity are not two separate approaches to fighting a pandemic. Herd immunity occurs when a large portion of a community (the herd) becomes immune to a disease, making the spread of disease from person to person unlikely. Vaccines are used to help populations reach herd immunity faster and without spreading illness. Advancements in vaccines are some of the greatest public health achievements over the last century. The only way we can build enough protection against the virus in our communities is if the majority of people receive the vaccine.
Vaccinations and herd immunity are not two separate approaches to fighting a pandemic. Herd immunity occurs when a large portion of a community (the herd) becomes immune to a disease, making the spread of disease from person to person unlikely. Vaccines are used to help populations reach herd immunity faster and without spreading illness. Advancements in vaccines are some of the greatest public health achievements over the last century. The only way we can build enough protection against the virus in our communities is if the majority of people receive the vaccine.
How was the adenovirus-based vaccine produced and tested so quickly?
The vaccines for COVID-19 have been developed at a record-setting speed, but they still were thoroughly tested to meet rigorous safety and efficacy standards. Before it is made widely available, any vaccine needs to be first studied in clinical trials. Then it is reviewed by an agency that oversees the safety and effectiveness of medical products. In the United States, this is done by the Food and Drug Administration (FDA). Starting a clinical trial for any medical intervention requires a research team, adequate funding and resources, and enough initial patients and data to properly plan the study. It’s a daunting task and is often why research and development take so long. Because this disease is a global health emergency, funding has been quickly directed toward reducing many of these barriers. The goal is to treat this dangerous disease as soon as possible, and as COVID-19 infection rates increased through 2020, researchers were able to gather a lot of data and eager volunteers for clinical trials.
What is Emergency Use Authorization?
During a declared public health emergency, such as the COVID-19 pandemic, the FDA can issue an Emergency Use Authorization (EUA) to provide access to medical products that may be used when there are no adequate, approved, and available alternatives. Under an EUA, the FDA makes a product available to the public based on the best available evidence, without waiting for all the evidence that would be needed for FDA approval. When evaluating an EUA application, the FDA carefully balances the potential risks and benefits of the products. The vaccines that have been granted EUA status in the United States are the mRNA vaccine developed by Moderna, the mRNA vaccine developed by Pfizer/BioNTech, and the adenovirus-based vaccine developed by J & J.
How do the vaccines currently authorized for emergency use compare?
In the U.S. there are currently two different mRNA vaccines, and one adenovirus-based vaccine that have received emergency use authorization for COVID-19 from the FDA. More vaccines authorized for emergency use means more people can get vaccinated sooner. The adenovirus-based vaccine does not need to be kept as cold as the mRNA vaccines, which makes it easier to distribute while the mRNA vaccines are easier to make compared to the adenovirus-based vaccine, which needs a viral vector to deliver genes to the cells. All the vaccines have provided protection against COVID-related hospitalizations and deaths.
Where can I find additional information?
The Centers for Disease Control and Prevention (CDC),the U.S. Food and Drug Administration (FDA), and the World Health Organization (WHO) offer credible resources about COVID-19 and mRNA vaccines for COVID-19.
Was this information helpful? If so, please share! All ASGCT Patient Education resources are free to use by sharing on social media, embedding the video, or simply linking to this page! Please credit The American Society of Gene and Cell Therapy.